
It’s 9:47 AM at a busy pediatric clinic.
The waiting room is already full. A toddler with a fever. A teenager here for a sports physical. A newborn coming in for a well visit. Phones are ringing, parents are asking questions and in the back office, someone is staring at a claim that just got denied… again.
If you have ever worked in pediatric billing or in a practice, this probably feels familiar.
Because here is the truth: pediatric billing isn’t just billing, it’s a constant balancing act between accuracy, compliance, and speed. And in 2026, with evolving payer rules and coding updates, the margin for error is smaller than ever.
That’s exactly why we put together this pediatric billing cheat sheet, not as a dry list of codes, but as a practical, real-world guide you can actually use.
The Moment Everything Clicks (Or Falls Apart)
Let’s start with a common scenario.
A 5-year-old comes in for a well-child visit. During the exam, mom mentions the child has been coughing for three days. The provider evaluates both.
Simple enough, right?
Not exactly.
From a pediatric coding cheat sheet perspective, this visit now involves:
- A preventive visit
- A problem-oriented visit
- Possibly a procedure (like a rapid strep test)
And if coded incorrectly? You risk:
- A denied claim
- Lost revenue
- Or worse; compliance issues
This is where understanding pediatric billing codes becomes critical.
The Core of Pediatric Billing (Your Everyday Codes)
Think of your pediatric CPT codes list as your daily toolkit. These are the codes you will use over and over again.
Preventive Visits (Well-Child Exams)
These are the backbone of pediatric care:
- 99381–99385 → New patients
- 99391–99395 → Established patients
But here’s what many teams overlook:
These codes are age-specific.
A wrong age bracket = an automatic denial.
Sick Visits (E/M Codes)
When a child comes in with a concern:
- 99202–99205 → New patients
- 99212–99215 → Established patients
In 2026, coding is driven by:
- Medical decision making (MDM)
- Time spent
Undercoding is one of the biggest revenue leaks in pediatric practices.
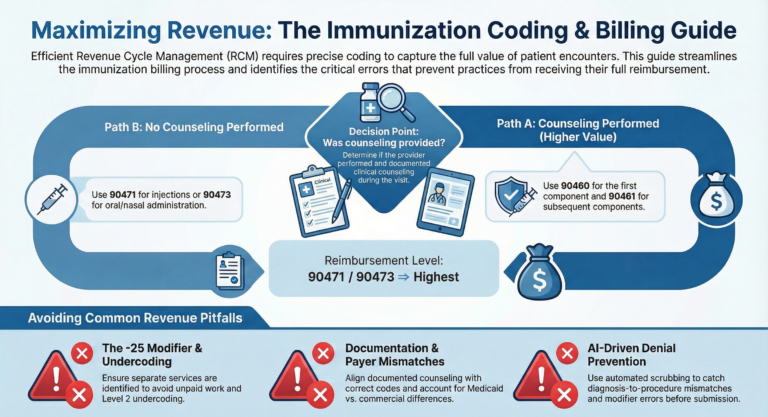
Immunizations (Where Most Mistakes Happen)
Vaccines are routine – but billing them correctly isn’t.
- 90460 → First vaccine with counseling
- 90461 → Each additional component
- 90471–90474 → Without counseling
Here is the catch:
If the provider documents counseling, you must use 90460/90461.
Miss that? You are leaving money on the table.
Developmental & Behavioral Screenings
These are more important than ever in pediatrics:
- 96110 → Developmental screening
- 96127 → Behavioral/emotional assessment
Some payers reimburse generously. Others bundle them.
Knowing the difference is key.
Common Office Procedures
These show up daily:
- 87880 → Rapid strep
- 94640 → Nebulizer treatment
- 92551 → Hearing screening
- 99173 → Vision screening
They seem simple; but missing documentation can kill reimbursement.
Is your practice leaking revenue on daily procedures?
Small codes like hearing screenings and nebulizer treatments add up to thousands in lost annual revenue if missed. Don’t let paperwork eat your profits. Let BillVolt’s pediatric specialists perform a free 10-point billing audit to find your missing revenue.
The “Wait… Can We Bill That?” Moment
Back to our 5-year-old patient.
Yes, you can bill both the preventive visit and the sick visit.
But only if you do it right.
The Rule:
- Add modifier -25 to the sick visit E&M code
- Ensure documentation clearly separates the two services
If not? The payer will bundle it, and you won’t get paid.
This is one of the most common mistakes we see when reviewing pediatric practices.
Where Most Practices Lose Money
After working with clinics across the country, one thing is clear:
It’s not that teams don’t know coding it’s that the details get missed in the chaos of a busy day.
Here are the biggest pitfalls in pediatric billing:
❌ Missing Modifier -25
You did the work… but didn’t get paid for it.
❌ Wrong Vaccine Coding
Counseling documented…. but billed incorrectly.
❌ Undercoding Visits
Providers spend 30 minutes…. but bill a level 2.
❌ Ignoring Payer Differences
Medicaid vs commercial plans can vary significantly.
The Reality of 2026: It’s Getting More Complex
Payers are tightening rules. Audits are increasing. And documentation requirements are more detailed than ever.
That’s why having a reliable pediatric coding cheat sheet isn’t optional anymore; it’s essential.
But even with the best cheat sheet, execution matters.
A Quick Reality Check
Ask yourself:
- Are your claims getting denied more than they should?
- Are you confident your vaccine coding is accurate?
- Are providers documenting enough to support billing?
- Is your billing team providing you with the support you need?
If you hesitated on any of these, you are not alone.
How BillVolt Helps Practices Stay Ahead
At BillVolt, we work with pediatric practices every day that are dealing with:
- High denial rates
- Underpayments
- Confusing payer rules
- Credentialing delays
And we fix it.
We don’t just do billing – we:
- Audit your current workflows
- Identify revenue leaks
- Optimize your coding process
- Train your team
👉 If you want to reduce denials and actually get paid for the work you are already doing, it’s time to talk. Contact BillVolt today.
Final Thoughts: It’s Not Just About Codes
At the end of the day, pediatric billing codes are just tools.
What really matters is:
- Knowing when to use them
- Documenting correctly
- And staying ahead of changing rules
Because behind every claim is:
- A child who needed care
- A provider who delivered it
- And a practice that deserves to be paid; accurately and fully
Ready to Simplify Your Pediatric Billing?
If your team is overwhelmed, or you just want a second set of eyes on your billing process. Reach out to BillVolt and let’s make your pediatric billing smoother, cleaner, and more profitable. We will handle the complexity, so you can focus on care.
Frequently asked questions (FAQs)
Frequently Asked Questions About Pediatric Billing and Coding
Can I bill a well-child check (99391-99395) and a sick visit (99212-99215) on the same day?
Yes, provided both services are distinct and medically necessary. You must append Modifier -25 to the sick visit (E/M) code and ensure your documentation clearly separates the preventive exam from the problem-oriented evaluation.
What is the difference between 90460 and 90471 for vaccines?
Use 90460 (and +90461 for additional components) when a physician or qualified healthcare professional provides clinical counseling to the parent. Use 90471–90474 for vaccine administration when no counseling is documented.
How has pediatric E/M coding changed in 2026?
Coding is now strictly driven by either Medical Decision Making (MDM) or Total Time spent on the date of the encounter. Under-coding level 4 visits (99214) as level 3 (99213) remains the most common "silent" revenue leak in pediatric practices.
Is developmental screening (96110) always reimbursed separately?
While most commercial payers and Medicaid plans recognize 96110 as a separate service, some "value-based" contracts in 2026 are attempting to bundle these into the well-visit. It is vital to track your contracts to ensure you aren't providing these assessments for free.
Why are my pediatric claims being denied for "Age/Linkage" errors?
Pediatric CPT codes (especially 99381–99385) are age-stratified (e.g., under 1 year, 1–4 years). In 2026, automated payer systems instantly reject claims where the patient's date of birth does not match the specific age bracket of the CPT code submitted.

