If you have worked in medical billing long enough, you already know this: IONM billing is not straightforward.
Between time-based codes, physician supervision rules, and payer-specific policies, even experienced billing teams can run into denials or compliance issues. The frustrating part? Most of these problems are avoidable with the right understanding and processes in place.
This guide is designed to break IONM billing down in a way that actually makes sense; no jargon overload, no textbook language; just clear, practical insight you can use in real workflows.
What is IONM and Why it Matters for Billing
Intraoperative neuromonitoring (IONM) is used during surgery to keep an eye on the patient’s nervous system in real time. The goal is simple: help surgeons avoid causing neurological damage.
You will typically see IONM used in:
- Spine surgeries
- Brain procedures
- ENT cases
- Certain vascular surgeries
From a billing perspective, what makes IONM unique is that it’s not just a test, it’s a continuous, real-time service involving:
- A technologist running the monitoring
- A physician interpreting the data live
And that “real-time” element is where most billing rules come from.
Why IONM Billing Gets Complicated
IONM isn’t like billing a standard procedure or office visit. It comes with a few layers that make things tricky:
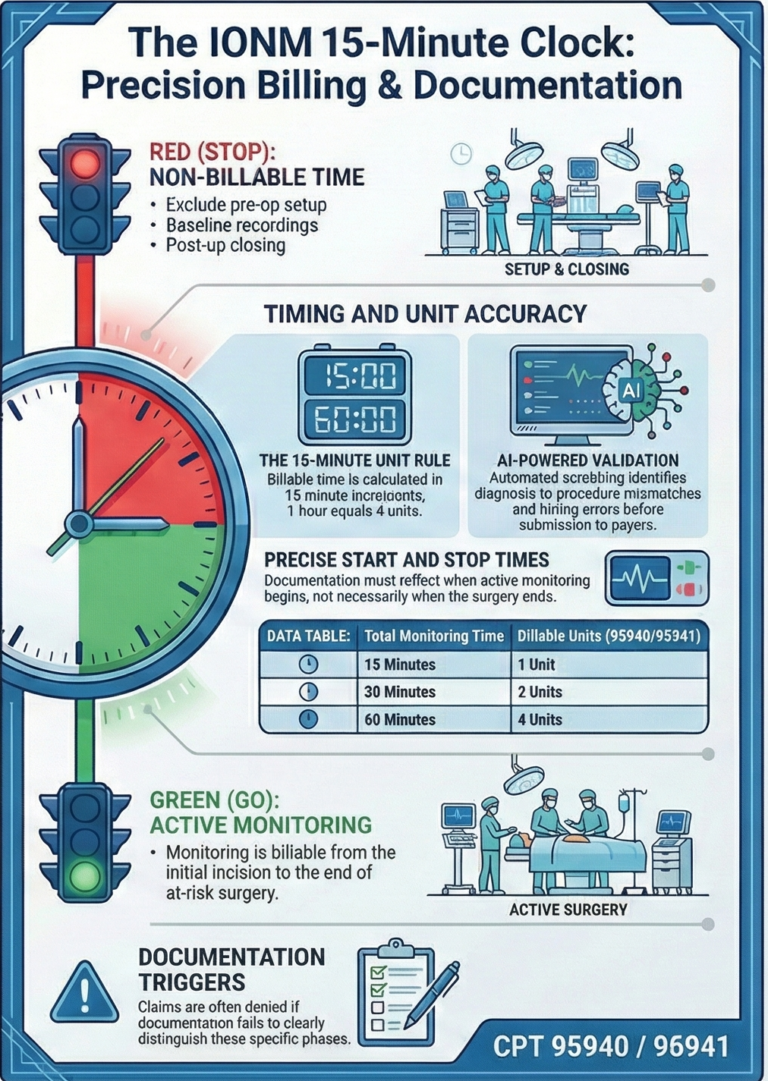
- It’s billed in 15-minute time blocks
- It requires active physician involvement
- There are limits on how many cases a physician can supervise at once
- Every payer seems to have slightly different expectations
Miss any one of these, and you are likely looking at denials, reduced payments, or audit risks.
Understanding the Core CPT Codes
At the center of IONM billing are two primary CPT codes:
- 95940 – Used when the physician is physically present in the operating room
- 95941 – Used when the physician is monitoring remotely
Here is the key point:
You cannot bill both codes for the same case. You must choose one based on how the service was delivered.
On top of that, you may also bill additional codes depending on what type of monitoring is performed (like EMG or evoked potentials). But those only work if they’re properly supported and not restricted by coding edits.
Is your IONM coding audit-ready?
One wrong modifier or a mismatched time-block can trigger a full payer audit. Don’t leave your compliance to chance. Let BillVolt review your IONM coding workflow today.
Time-Based Billing: Where Accuracy Really Matters
IONM billing lives and dies on time documentation.
You are billing in 15-minute increments, but not all time counts.
When billing should start:
- After baseline readings are completed
- When active monitoring actually begins
When it should stop:
- When monitoring is no longer needed
- Not necessarily when the surgery ends
This is where many teams slip up. If your documentation doesn’t clearly show:
- Start time
- Stop time
- Continuous monitoring
…you are giving payers a reason to deny the claim.
Physician Supervision and Concurrency (A Big One)
One of the most heavily scrutinized areas in IONM billing is concurrency, meaning how many surgeries a physician is monitoring at the same time.
According to the Centers for Medicare & Medicaid Services and most major payers:
- Physicians are generally expected to monitor no more than 3 cases simultaneously
If that number goes higher:
- Reimbursement may be reduced
- Claims may be denied
- It can raise compliance concerns during audits
This isn’t just a billing issue, it’s a risk management issue.
Documentation: Your Best Protection
If there is one thing that protects your revenue in IONM billing, it’s documentation.
Strong documentation should clearly show:
- What procedure was performed
- What monitoring techniques were used
- Baseline results
- Any changes during surgery
- Communication with the surgeon
- Exact monitoring times
- Physician involvement throughout
Think of it this way:
If an auditor picked up your report, could they clearly see that the service was necessary and properly performed? If not, it needs work.
Medical Necessity: Don’t Skip This Step
Not every surgery qualifies for IONM billing.
For a claim to be paid:
- The service must be medically necessary
- It must be ordered by the surgeon
- It must include real-time interpretation
Billing IONM for procedures that don’t meet these criteria is one of the fastest ways to trigger denials, or worse, audits.
Common Mistakes That Cost You Money
Let’s keep this real; these are the issues we see all the time:
- Billing both primary codes (95940 + 95941) together
- Guessing or rounding time instead of documenting it
- Overloading physicians with too many concurrent cases
- Submitting claims without clear physician involvement
- Skipping medical necessity checks
None of these are small errors. Over time, they can lead to significant revenue loss.
Stop the IONM Revenue Leak
If your team is rounding time or struggling with concurrency limits, you’re losing earned income. BillVolt specializes in maximizing 15-minute increment reimbursements for complex surgical cases.
Facility vs. Professional Billing: Know the Difference
IONM billing often involves more than one party.
- The physician bills for interpretation
- The facility or provider group may bill for the technologist
Depending on your setup:
- Hospitals may bundle services
- Independent IONM companies may bill separately
If roles and agreements aren’t clearly defined, billing can quickly become inconsistent.
Practical Tips to Improve Your IONM Billing Process
If you want cleaner claims and fewer denials, focus on these:
- Use structured reporting templates
- Track monitoring time in real time (not after the fact)
- Monitor physician concurrency closely
- Stay updated on payer-specific rules
- Run regular internal audits
Small process improvements here can make a big difference in reimbursement.
Where IONM Billing Is Headed in 2026 Onwards
Payers are paying closer attention to IONM than ever before.
We are seeing:
- Increased audits
- Stricter enforcement of supervision rules
- More focus on documentation quality
The takeaway?
The margin for error is shrinking.
Organizations that tighten their processes now will be in a much stronger position moving forward.
Final Thoughts
IONM billing isn’t impossible; but it does require attention to detail.
When done right, it can be a reliable and valuable revenue stream. When done wrong, it quickly becomes a source of denials and compliance headaches.
At BillVolt, we focus on simplifying complex billing challenges like IONM so providers don’t have to navigate them alone.
Want help cleaning up your IONM billing process?
Visit 👉 www.billvolt.com and connect with our team.
Frequently asked questions (FAQs)
Frequently Asked Questions About Intraoperative Neuromonitoring (IONM) Billing
What is the difference between CPT 95940 and 95941?
CPT 95940 is used when the monitoring physician is physically present in the operating room or the same facility. CPT 95941 is used for remote monitoring (telemedicine). It is a major compliance error to bill both for the same procedure; you must choose the one that reflects the physician's actual location.
How many cases can a physician monitor concurrently in 2026?
According to CMS and most major private payers, a physician is typically limited to monitoring three (3) cases simultaneously. Exceeding this "3-to-1" ratio can lead to automatic claim denials or serious compliance red flags during an audit.
When exactly should the 15-minute billing clock start for IONM?
Billing should only begin after baseline readings are completed and active, continuous monitoring of the surgical procedure has started. Pre-operative setup and baseline recording time are generally not billable as part of the intraoperative time blocks.
Can we bill for IONM during every spine or brain surgery?
No. To be reimbursable, IONM must meet the payer's definition of medical necessity. This usually requires a surgeon's order and a documented risk of permanent neurological damage that the monitoring is designed to prevent. Always check payer-specific LCDs (Local Coverage Determinations).
What documentation is required to support IONM time-based codes?
Documentation must include precise start and stop times, a log of any significant neurological events or communications with the surgeon, and a summary of the physician’s real-time interpretation throughout the case. "Estimated" or "rounded" times are frequently rejected during audits.